
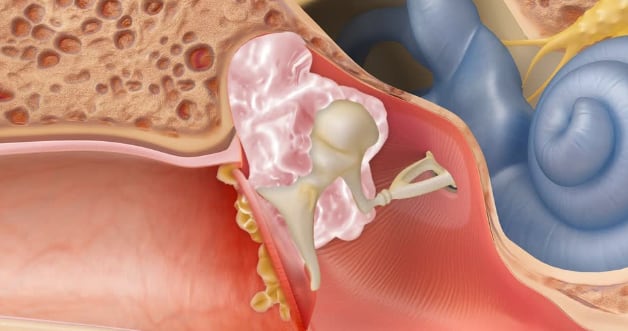
A cholesteatoma is skin growth occurring in the middle ear or mastoid bone behind the eardrum. It is sometimes also called a skin cyst. This is caused by an ingrowth of the skin of the eardrum in most cases.
Skin is always regenerating. Once your skin cells die everywhere else in your body, they flake off or exfoliate. If there is skin is in the middle ear, there is nowhere for it to escape as it enlarges. The cholesteatoma growth is slow, but over time skin can erode bone and damage nerves. Cholesteatomas can also become chronically infected, leading to infections and foul-smelling drainage.
For most people, it occurs because their eustachian tube is not working properly. Your eustachian tube is supposed to equalize pressure between your middle ear and the outside world. If it is not equalizing pressure the air in your middle ear is absorbed by your body and negative pressure results, leading to your eardrum being sucked in (retracted). Since the outer layer of your eardrum is skin, this can lead to that skin becoming trapped on the wrong side of the eardrum. There are several other less common causes.
 What are the normal symptoms from a cholesteatoma?
What are the normal symptoms from a cholesteatoma?The most common symptoms are ear drainage, hearing loss, and ear fullness. Sometimes ringing (tinnitus) can occur because of the hearing loss. Infrequently it can cause pain.
No. There is no possibility of it becoming cancer.
Cholesteatomas can be dangerous. There are a lot of important structures around the middle ear that could potentially be damaged. Cholesteatomas grow slowly, but if left unchecked can have severe consequences.
Uncommon complications that can occur if left untreated:
In order to remove a cholesteatoma, surgery is necessary. Initially, cholesteatomas often present when they are infected, and they are treated with either oral or topical antibiotics. This can alleviate the initial symptoms, yet surgery is still recommended to avoid damage to critical structures in and around the ear.
A CT scan is usually ordered to determine whether the cholesteatoma has eroded any critical structures, such as the inner ear, facial nerve, brain cavity, and to help with surgical planning. Sometimes an MRI is also needed.
All three goals are always sought, however depending on the severity of the cholesteatoma, they cannot always be achieved.
The surgery is performed under general anesthesia. A small incision is usually made behind the ear, but that can sometimes be avoided if the cholesteatoma is caught early enough. Ear endoscopes are often used to help remove cholesteatoma from hard to reach parts of the middle ear.
There are three possibilities outcomes for the initial surgery:
You will receive narcotic pain medication just in case, however most patients don’t need it. Tylenol and ibuprofen are usually enough to manage the pain from surgery. Recovery means different things to different people, and everyone bounces back at different rates. In general, after a couple of days of recovery patients are back to their normal routine. You can shower the day after surgery – if there is an incision it is ok to get it wet, but do not scrub directly on it. It helps healing to apply plain Vaseline daily to the incision.
Please call one of our locations: West Joliet 815-725-1191, New Lenox 815-717-8768, and Morris 815-941-1972 to schedule an appointment.
Contact Us Today!