
 What is a vestibular schwannoma?
What is a vestibular schwannoma?A vestibular schwannoma, also known as an acoustic neuroma, is a benign tumor of a balance nerve between your ear and brain. It originates from Schwann cells which cover this nerve. If you think of the nerve like a copper wire with rubber covering, Schwann cells are the equivalent of the rubber covering.
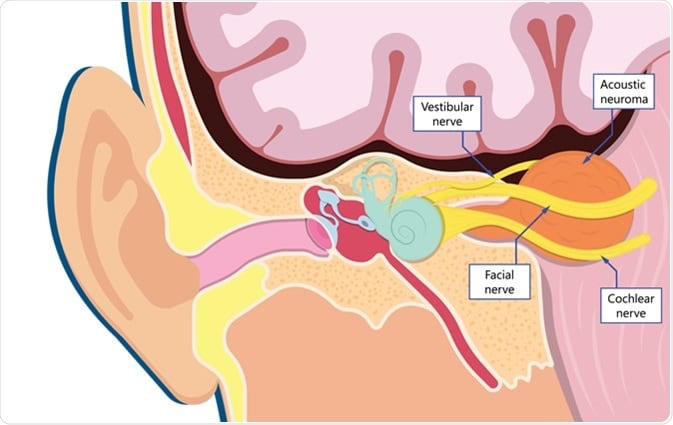
Depending on the size, it is in the internal auditory canal +/- the cerebellopontine angle. If you start in your ear canal and go straight toward the center of your head, on the other side of the inner ear you would be in the internal auditory canal. It houses four important nerves – the facial nerve (controls muscles on that side of your face), the cochlear nerve (hearing), and two vestibular nerves (balance). The cerebellopontine angle is a space between the internal auditory canal and your brain (specifically the pons, cerebellum, and temporal lobe). There are several other important nerves which go through this space.
No, and it cannot become cancer.
Usually it is not, however if it grows to be large enough it can be.
The symptoms are caused by compression of nerves the tumor pushes against.
How can you know that it is a vestibular schwannoma without a biopsy?
It is true that there is no way to know definitively without a biopsy, however we can often tell based on the MRI you had. When there is a tumor in this part of the brain 85% are vestibular schwannomas, 10% are meningiomas (also benign), and the remaining 5% are a variety of very rare tumors.
Usually random chance. There is a genetic disease called neurofibromatosis type 2 where patients grow vestibular schwannomas on both sides, but this is extremely rare.
Every vestibular schwannoma is different. It is generally a slow growing tumor with an average growth rate of 1-2mm in diameter per year. However, some tumors do not grow after they are discovered, and some are more aggressive.
This is very hard to predict in the short term. Some patients lose their hearing gradually and some suddenly. Without treatment, by ten years after diagnosis over 90% of patients are functionally deaf in the involved ear. The degree of hearing loss is more accurately predicted by the precise location of the tumor, not the size. Once you have lost your hearing, it will never come back.
There are three potential options for managing a vestibular schwannoma. Not all options are appropriate for all patients. Your doctor will tell you which option(s) are appropriate for you.
Observation with regular MRI surveillance – This is appropriate for some smaller tumors, particularly for older patients. If this option is chosen another MRI would be performed in six months. If there is no or minimal growth the next MRI would be one year later. If the tumor does grow it may later become necessary to pursue intervention. Without surgery, almost all patients are functionally deaf in their involved ear by 10 years after diagnosis.
Stereotactic radiotherapy – This is a radiation treatment where in one outpatient session a radiation oncologist will deliver targeted beams with a linear accelerator. This treatment cannot be performed in the Joliet area because none of the hospitals have the proper machinery, so you would be referred towards the city. The goal of this treatment is to slow growth or shrink the tumor, not to remove it. For the first 6-18 months following treatment the tumor will swell and increase in size, so this cannot be performed on large tumors. There is a risk of imbalance and/or facial weakness following this treatment, however it is easier to tolerate than surgery and does not require a hospital stay. This is not considered a hearing preservation treatment – most patients still lose their functional hearing within 10 years of treatment.
Surgical removal – This is a surgical procedure under general anesthesia using a microscope requiring a night in the intensive care unit with a 2-4 night hospital stay. Dr. Bartindale performs this surgery in conjunction with a neurosurgeon. The length of the surgery is highly variable depending on the size and location of your tumor. There are three potential approaches which can be used – translabyrinthine, retrosigmoid, and middle fossa. Certain approaches are best for certain tumors and Dr. Bartindale will discuss this with you. With the retrosigmoid and middle fossa approaches hearing can potentially be preserved. Lumbar drains and fat grafts from the abdomen are sometimes necessary.